

Reimagining Healthcare: Process Improvement for a Patient-Centric Future
By Maya El-Haj
If the healthcare sector is to shift towards a patient-centric model successfully, it will first need to break down and assess the processes. As we illustrate in our article “How Healthcare can Learn from Other Industries to Improve Patient Experience,” the root causes behind disconnected processes in healthcare are the misalignment among the different stakeholders in the ecosystem, the lack of unified operating models resulting in different KPIs, SLAs, and OLAs, and the lack of end-to-end ownership of patients’ journeys. Potentially, the disconnection in processes will cause an increase in lead time to resolve problems, which in healthcare could lead to a significant consequence that goes beyond the loss of a “customer.”
New Metrics’ Maya El-Haj sat down with Pablo Friedrich Lorenz, a Lean Six Sigma Black Belt with extensive experience implementing process change, to learn more about his work at the NHS Hospital Trust in the UK.
At New Metrics, we have seen the same challenges and opportunities that Pablo experienced throughout his healthcare engagements. We believe that a patient-centric model faces amplified customer experience challenges due to the multi-layered nature of the healthcare industry.
Maya El-Haj: From your experience, which point during the typical patient pathway at a health care center or hospital do you feel is currently the most overlooked in terms of an opportunity to improve the flow of the experience?
Pablo Lorenz: The initial engagement is often overlooked, and this is where the patient experience can be improved from the very start. A ‘Patient Pathway,’ the journey from initial engagement through to discharge, is not really at the forefront for many staff. Once the ‘journey’ starts, the interface between departments is usually not well managed. For example, the transfer from an outpatient clinic to a ward, or from a ward to the X-Ray department and back, can feel chaotic and give the patient the impression they are not a priority.
Maya El-Haj: Where do you feel the most significant improvements could be made to the patient pathway?
Pablo Lorenz: I believe the most critical areas a healthcare provider can improve are the discharge process and aftercare. These are the most significant. Changing the way this portion of the journey is delivered leads to overall better long-term recovery. There is a lot of research about the benefits of early recovery and early mobilization of patients. As a result, the recovery process is accelerated, and the overall patient experience is also improved.
Maya El-Haj: From a commercial and operational perspective, do you feel that there is greater ‘value’ in ensuring a patient is fully recovered before discharging them rather than releasing them early and having to readmit?
Pablo Lorenz: One way to ease the demands on the hospital is through the early discharge of patients. It may seem counter-intuitive, but early discharge is advisable from an operational efficiency perspective and a recovery perspective. Early discharge does have to be carefully managed, though. The patient needs to be fully committed, and their situation needs to be assessed to ensure that the necessary home care can be provided after the discharge.
Maya El-Haj: How do you feel that ‘for-profit’ healthcare has impacted the standard of care? Both positively and negatively.
Pablo Lorenz: A responsible organization that puts the patient and the best possible outcome first will certainly generate more sustainable long-term efficiency and effectiveness as ‘side-effects’ without compromising care. However, if profitability is the overriding objective and at the forefront of management decisions, patient experience can very quickly get lost along the way.
Maya El-Haj: Do you feel the reliance on private practitioners to bridge the gap could be reduced? And how?
Pablo Lorenz: This is a risky approach. It is far more efficient to devise a permanent solution. If you must bridge a gap, it means there is a gap in the first place. Deploying private practitioners is a very costly and temporary approach. Any gaps should be closed systemically and sustainably with permanent staff.
Maya El-Haj: How do you believe health care providers can strike a healthy balance between fulfilling operational KPIs and cost-effectiveness vs. providing the best level of care and a superior patient experience?
Pablo Lorenz: Every healthcare provider has limited resources, both financially and staff-wise. Therefore, it is important to ensure full awareness of the need to balance KPIs. It starts with the understanding of the factors that positively influence the patient experience. Capturing data and analyzing the results is critical in this regard. Otherwise, you might find yourself investing in certain aspects that you perceive as driving patient experience while they aren’t. At the same time, it is just as important to create awareness and reassure medical staff that efficiency and cost-effectiveness do not equal cost-cutting and reducing medical care.
Maya El-Haj: If you were to redesign a healthcare KPI scorecard, what would you place at the center as a core metric?
Pablo Lorenz: I think this is exactly why you have multiple measures on a KPI scorecard. It is easy to be either fast, good, or cheap, but the real challenge is in the combination of these measures. Overall, it depends on the strategy of the healthcare provider where the focus is set. I think it should be centered around patient well-being, supported by measures around efficiency and effectiveness to ensure that the superior patient experience can be delivered to as many patients as possible.
Implementing process improvements can have startling results. Streamlining scheduling, implementing data-driven communication processes, and improving documentation have seen tangible improvements at NHS Hospital Trust in the UK.
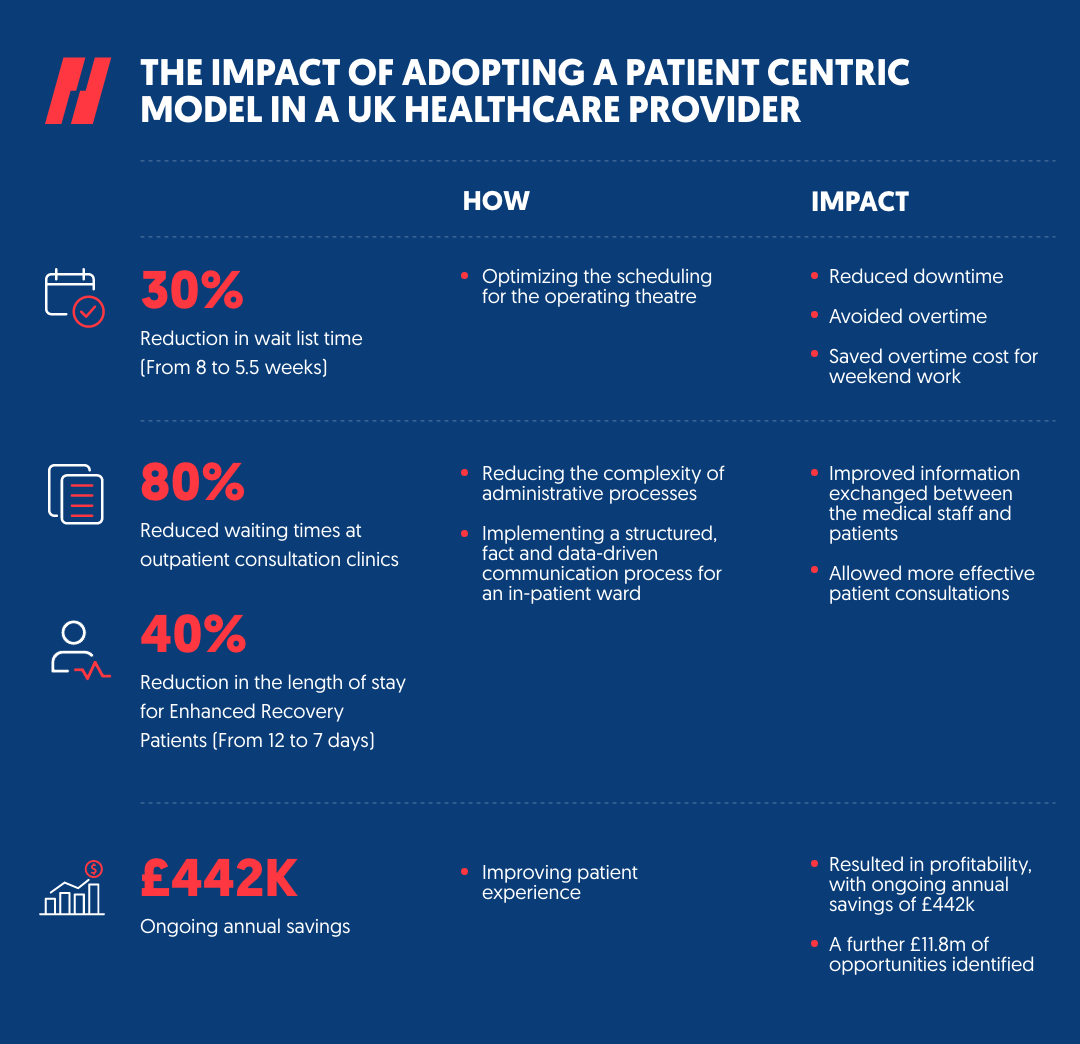
Optimizing the scheduling for the operating theatre reduced downtime and avoided overtime. That has shortened the waitlist time by around 30%, from eight weeks to 5.5, and saved overtime costs for weekend work.
Implementing a structured, fact and data-driven communication process for an in-patient ward improved consistency and quality of information exchanged between doctors, nurses, patients, and relatives across shifts. The optimized documentation process also reduced the complexity of the administrative process by 80%, reduced waiting times at outpatient consultation clinics, and allowed more effective patient consultations.
The length of stay for Enhanced Recovery Patients also dropped by 40% – from 12 days to 7 days.
And finally, proving that improved patient experience can lead to profitability, the efficiency improvements Pablo and his team introduced resulted in ongoing annual savings of £442k, with a further £11.8m of opportunities identified.
Today more than ever, healthcare industry players must put their efforts into adopting a patient-centric model to improve the overall patient experience and reap operational and financial benefits.